When Psychosis Looks Like Autism: A Parent's Guide
By Pand Health
When Psychosis Looks Like Autism: A Parent’s Guide
First episode psychosis masquerading as autism is defined as a condition where early psychotic symptoms so closely resemble autistic behaviors that clinicians and parents mistake one for the other. Both conditions share social withdrawal, unusual speech, and repetitive movements, making the diagnostic picture genuinely confusing. The formal clinical term for this overlap is “differential diagnosis between autism spectrum disorder (ASD) and schizophrenia spectrum disorders (SSD),” and getting it right matters enormously. A missed psychosis diagnosis delays treatment that can prevent long-term cognitive decline. This article gives parents a clear framework for understanding what separates these two conditions and when to push for a second look.
What are the overlapping symptoms between first episode psychosis and autism?
Parents often notice the same cluster of behaviors whether their child has autism or early psychosis. Both conditions can produce social withdrawal, reduced eye contact, unusual speech patterns, and repetitive movements. That overlap is exactly why first episode psychosis masquerading as autism happens so frequently in clinical settings.
The behaviors that cause the most confusion include:
- Social withdrawal. A child pulls away from friends and family in both conditions, but the reason differs fundamentally.
- Repetitive or stereotyped movements. Hand-flapping, rocking, and rigid routines appear in autism and can also emerge in early psychosis.
- Unusual sensory responses. A child with psychosis may react to hallucinated sounds or sensations in ways that look identical to autistic sensory sensitivities.
- Odd or disorganized speech. Both conditions can produce tangential thinking, echolalia-like patterns, or flat affect.
- Rigid beliefs and inflexible routines. Psychosis can generate fixed, unusual ideas that look like autistic insistence on sameness.
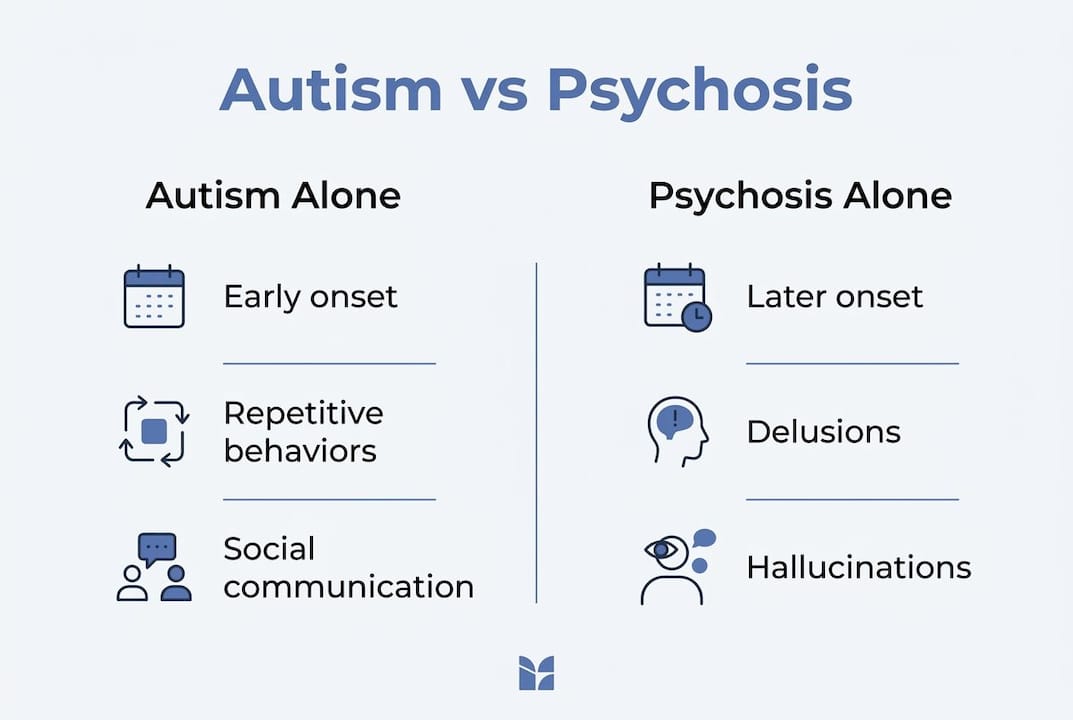
The timing of onset is the single most useful clue. Early-onset psychosis symptoms typically appear after age 8, not from early childhood. Autism, by contrast, is a lifelong neurodevelopmental condition with signs present from infancy or toddlerhood. That developmental timeline is the first thing to examine.
Social withdrawal in schizophrenia is a defensive retreat, a child pulling inward to manage a destabilizing inner experience. In autism, social isolation reflects an innate difference in social attunement, not a response to distress. That distinction changes everything about how you interpret the behavior.
Pro Tip: Track your child’s behavior over time, not just in a single appointment. A cross-sectional snapshot misses the most important diagnostic signal: whether symptoms are new and worsening, or lifelong and stable.
How can parents and clinicians distinguish early signs of psychosis from autistic traits?
Distinguishing early signs of psychosis from autism requires looking at four specific dimensions: onset timing, symptom quality, developmental history, and cognitive change.
- Establish a developmental baseline. Ask when the behaviors first appeared. Autism traits are present before age 3 in most cases. New behavioral changes emerging in a child who previously developed typically point toward psychosis or another acquired condition.
- Look for hallucinations and delusions. These are psychosis-specific. A child describing voices, seeing things others cannot see, or expressing fixed false beliefs (such as believing they are being watched or poisoned) is showing psychotic symptoms, not autistic traits.
- Note the quality of delusions. Psychosis in autistic youth tends to produce concrete, systematized delusions tied to the child’s existing interests or sensory world, rather than the complex paranoid delusions seen in adult schizophrenia. This makes them easier to miss.
- Watch for cognitive decline. A child who was previously keeping up academically and then begins to struggle with attention, memory, or processing speed may be experiencing psychosis-related cognitive impairment, not a static neurodevelopmental profile.
- Gather collateral history from multiple sources. Teachers, grandparents, and coaches often notice changes that parents, who see the child daily, may normalize. Longitudinal developmental history and collateral family input are the most reliable tools for reducing misdiagnosis risk.
- Screen for sleep disturbances, mood shifts, and new aggression. These are common early markers of psychosis and are not typical features of autism alone.
A common pitfall is misinterpreting inner speech as hallucinations. Many autistic children talk to themselves or narrate their thoughts aloud. The clinical difference is that true hallucinations are experienced as external, coming from outside the child’s own mind. Asking the child directly, in age-appropriate language, whether the voice feels like their own thought or like someone else speaking, can clarify this.
Pro Tip: Keep a written log of behavioral changes with dates. Note what changed, when it started, and whether it has progressed. This documentation gives any clinician the longitudinal picture they need to make an accurate diagnosis.
What is known about autism and psychosis co-occurrence?
Autism and psychosis are not mutually exclusive. Autistic individuals carry elevated psychosis risk compared to neurotypical peers, with psychosis typically emerging in adolescence or early adulthood. This means a child can have both conditions simultaneously, which creates a more complex clinical picture than either diagnosis alone.
Research on cognitive profiles reveals a specific pattern when both conditions co-occur. The table below summarizes the key differences and overlaps.
| Feature | Autism alone | First episode psychosis alone | Co-occurring ASD and psychosis |
|---|---|---|---|
| Social withdrawal | Lifelong, trait-based | Recent, defensive | Both patterns present |
| Recognition memory | Often preserved or strong | Impaired | Preserved (ASD strength retained) |
| Processing speed | Variable | Significantly impaired | Impaired (psychosis effect dominant) |
| Delusions | Absent | Complex or paranoid | Concrete, tied to interests |
| Onset timing | Early childhood | Adolescence or later | Adolescence, on ASD baseline |
| Response to treatment | Behavioral and educational | Medication and therapy | Requires both, tailored approach |
Patients with co-occurring autism and first episode psychosis show an additive cognitive profile. They retain ASD-associated strengths like recognition memory while also experiencing psychosis-related impairments in processing speed and attention. This pattern is distinct from either condition alone and requires a treatment plan that addresses both simultaneously.
Autistic features within first episode psychosis identify a subgroup of patients with greater cognitive and functional challenges. These patients need more intensive, personalized intervention. A standard first episode psychosis protocol designed for neurotypical patients will not fully address their needs.
The clinical implication is direct: if your child has an existing autism diagnosis and begins showing new behavioral changes, do not assume the changes are part of autism. Psychosis requires its own evaluation and its own treatment pathway. Pandhealth’s autism and early psychosis care programs are specifically designed to assess and treat this kind of diagnostic complexity in teens and young adults.
Why might first episode psychosis be misdiagnosed as autism?
Misdiagnosis happens most often when clinicians rely on a single evaluation rather than a longitudinal picture. Cross-sectional symptom observation that ignores developmental history leads clinicians to mistake enduring neurodevelopmental traits for chronic psychosis, or vice versa. Both errors carry serious consequences.
The most common reasons for misdiagnosis include:
- Diagnostic shadowing. Once a child carries an autism label, new symptoms get attributed to autism rather than evaluated independently. Clinicians stop looking for other explanations.
- Overlapping surface behaviors. Repetitive movements, flat affect, and social withdrawal look the same regardless of cause. Without knowing the child’s history, a single observation cannot distinguish them.
- Age of the evaluating clinician’s experience. Clinicians who primarily see adult psychosis patients may not recognize how differently psychosis presents in children and adolescents.
- Underreporting by the child. Children with autism may have limited insight into their own internal experiences. They may not report hallucinations because they lack the language or awareness to describe them.
- Parental normalization. Parents who have managed autism for years sometimes attribute new and alarming symptoms to “a bad phase” rather than recognizing them as a clinical change.
Periodic diagnostic reconsideration is the clinical standard when a child’s symptoms persist or worsen despite treatment. If your child is not improving as expected, that is a signal to request a full reassessment, not to increase the current treatment dose.
The risks of misdiagnosis are real. A child treated for autism who actually has psychosis will not receive antipsychotic medication, coordinated specialty care, or the early intervention that prodromal and first episode psychosis programs are designed to deliver. Every month of untreated psychosis carries a measurable cost to cognitive function and long-term outcomes.
Pro Tip: If your child’s behavior has changed significantly in the past 6 to 12 months and their current treatment is not helping, ask the treating clinician directly: “Have we ruled out psychosis?” That question alone can redirect the diagnostic process.
Pandhealth’s specialized care for youth with psychosis and autism
Pandhealth, based in Los Angeles, specializes in early intervention for teens and young adults ages 13–35 who are experiencing thought disorders, including cases where autism and psychosis overlap. The clinical team uses an augmented version of the evidence-based California OnTrack coordinated specialty care model, which combines psychiatry, medication management, cognitive remediation, family psychoeducation, and school or employment support.
When the diagnostic picture is unclear, Pandhealth’s multidisciplinary team conducts thorough evaluations that account for developmental history, cognitive profiles, and current symptom patterns. Parents who are asking “is it autism or psychosis?” deserve a clear, expert answer. Pandhealth’s early psychosis treatment program is built to provide exactly that, with personalized care pathways that address both conditions when they co-occur.
Key Takeaways
Distinguishing first episode psychosis from autism requires longitudinal developmental history, symptom onset timing, and cognitive profiling, not a single cross-sectional evaluation.
| Point | Details |
|---|---|
| Onset timing is the first clue | Autism traits appear in early childhood; psychosis symptoms typically emerge after age 8. |
| Social withdrawal has two meanings | In autism it is a lifelong trait; in psychosis it is a recent, defensive response to inner distress. |
| Co-occurrence is real and complex | Autistic youth carry elevated psychosis risk, and both conditions can be present simultaneously. |
| Cognitive profiles differ and combine | Co-occurring ASD and psychosis produces an additive pattern: retained memory strengths plus processing speed impairments. |
| Misdiagnosis is preventable | Longitudinal history, collateral reports, and periodic diagnostic review reduce the risk of missing psychosis in autistic youth. |
FAQ
What does “first episode psychosis masquerading as autism” mean?
It describes a situation where early psychotic symptoms, such as social withdrawal, repetitive behaviors, and unusual speech, closely resemble autism traits, leading to a missed or delayed psychosis diagnosis. The key distinction lies in the timing and trajectory of symptom onset.
Can a child have both autism and psychosis at the same time?
Yes. Autistic individuals carry elevated psychosis risk compared to neurotypical peers, and both conditions can be present simultaneously. Co-occurring autism and first episode psychosis produces a distinct cognitive profile that requires a tailored treatment approach.
What are the earliest signs of psychosis in a child?
Early signs include new social withdrawal, sleep disturbances, mood changes, declining school performance, and reports of hearing or seeing things others cannot. These symptoms emerging in a child who previously developed typically are a clinical red flag.
How is psychosis in autistic youth different from psychosis in neurotypical youth?
Psychosis in autistic youth more commonly features concrete, systematized delusions tied to the child’s existing interests rather than complex paranoid hallucinations. This presentation is easier to miss and requires clinicians experienced with both conditions.
When should a parent seek a specialist evaluation?
Seek a specialist evaluation when your child’s behavior changes significantly over weeks or months, when current treatment is not producing improvement, or when you observe possible hallucinations or fixed false beliefs. A multidisciplinary team with experience in both autism and psychosis provides the most accurate assessment.


